An interview with Former President of the SCCM, Jerry Zimmerman.
Former President of the SCCM, Jerry Zimmerman joined us on “Hills and Valleys” podcast at the recent Society of Critical Care Medicine Conference to share his insights on a variety of topics.
In this article:
- Who is Dr. Jerry J. Zimmerman?
- What is NADPH oxidoreductase?
- Why choose critical care medicine?
- Why is sepsis a problem?
- What is ICU Heroes Award?
- Can sepsis be prevented?
- What is the continuum of care?
- What is usual care in medicine?
- What is the ABCDEF bundle?
- What are new approaches in critical care medicine?
- Who is
Dr. Heatherlee Bailey?
About Hills and Valleys
Hills and Valleys is a podcast that uncovers stories from leaders in healthcare, tech, and everything in between. Straight from the heart of Silicon Valley, we give you a look at the good, the bad, and the future, one episode at a time. Brought to you by Potrero Medical.
Listen to the podcast on any of the platforms below, watch the full video interview, or continue reading this blog to see the transcript.
About Dr. Jerry J. Zimmerman, MD, PhD , Seattle Children’s Hospital
Jerry J. Zimmerman, MD,
He is Professor of Pediatrics and Anesthesiology at the University of Washington School of Medicine. Zimmerman has been chair of the Scientific Advisory Committee for Children’s Hospital Clinical Research Center since its inception and is a member of the Steering Committee for the Center for Clinical and Translational Research.
He is a charter member of the American College of Critical Care Medicine and is Treasurer of the Society of Critical Care Medicine and is a member of the Executive Committee.
With Bradley Fuhrman, Zimmerman is co-editor of the current premier textbook for the field, Pediatric Critical Care, now in its 4th edition. Additionally, Zimmerman serves on the editorial boards for Critical Care Medicine and Pediatric Critical Care
Dr. Zimmerman is interested in the disequilibrium between the systemic inflammatory response syndrome and compensatory anti-inflammatory response syndrome that occurs as an important aspect of pathophysiology in critical illness. He is interested in the integrated role of neurological, endocrinologic and inflammatory cross-talk, particularly involving reactive oxygen species and fatty acid-derived mediators and their effect on metabolism.
Follow him on Twitter @jerjohzimm
- Interviewer: Omar M. Khateeb, Director of Growth atPotrero Medical
- Interviewee: Dr. Jerry J. Zimmerman, Professor of Pediatrics and Anesthesiology at the University of Washington School of Medicine and Seattle Children’s.
Khateeb: Hi everyone. This is Omar M. Khateeb the Director of Growth at Potrero Medical and this is another episode of Hills and Valleys.
I’m at the beautiful Society of Critical Care Medicine here in San Diego, with the former president of the society, Dr. Jerry Zimmerman, who has had a very busy schedule but has been kind enough to sit down with us.
I’ll give you a little bit of background on him. He’s a professor of anesthesiology and pediatrics at the University of Washington. He has a variety of research interests, a very, very kind gentleman, and I’m gonna give him an opportunity to give us a little bit more color on his background.
Zimmerman: Thanks Omar. So I have been working in pediatric critical care medicine for over 30 years at the University of Wisconsin in Madison, and now at the University of Washington in Seattle.
So I have seen a lot of innovation, also a lot of research that unfortunately has not supported things that we thought were dogma in the past, but this is an exciting area of medicine in which you go to work and you come home and you know, you’ve made a difference and the other thing that’s fun about working in critical care is that new things, new technologies frequently filter through the ICU first and so it’s an exciting, albeit stressful environment to work, but we have the advantage of really going to work every day and seeing how we can make a difference.
Khateeb: It’s fantastic. Now, of your research interests, I saw that you’ve done quite a lot of work with pediatrics and specifically in sepsis. Can you tell us a little bit more about that?
Zimmerman: So yes, I have been a researcher in sepsis, I guess essentially, since the beginning of my career, before going into medicine. I was actually a cancer researcher and I actually worked on this enzyme, if we want to get geeky for a second.
Khateeb: We love that here!
Zimmerman: NADPH oxidoreductase.
It is actually an enzyme that is membrane-bound and it generates superoxide, which is the parent oxyradical metabolite that can be metabolized hydroxyl radical and hydrogen peroxide and hypochlorous acid, lots of things, not only direct injury, but very important cellular signaling and I did that as part of my cancer research work when I became a doctor..
And
Neutrophil is the like infantry person that shows up before just about anything else, maybe compliment, but this generation of oxygen radical metabolites is a key aspect of a host of response syndromes involving inflammation, sepsis is typical, but other things as well.
So that’s sort of how I got into it as a physician and over the years, I have been involved with diagnosing sepsis. This is actually the neatest, the sexiest research that I’m involved in right now, in Seattle; treating sepsis. We are currently about to launch, hopefully, a clinical interventional trial related to steroids, and then very interested in long-term outcomes after sepsis.
In fact, right now we are waiting for decisions trying to get the results of a long-term follow-up of children after septic shock and their quality of life, the burden and the duration of that morbidity following pediatric sepsis. So I really am interested in the Continuum of Care and that’s the focus of this meeting, for children with sepsis.
Khateeb: Interesting. It’s fascinating to hear you get so excited about it when we think about sepsis, and this is a disease that can be caused by so many different things and really is a true black box in medicine.
And so do the complicated, sophisticated problems like that, is that what drew you into sepsis and perhaps critical care medicine?
Zimmerman: I think what drew me into critical care medicine now…I was originally going to be an adolescent medicine physician and it turned out during pediatrics, my first rotation was in the PICU and I had this rotation when I said, “This is what I want to do.” It is not that adolescent medicine isn’t important at all, that’s not the point. I got so worked up and excited about actually making a difference in real-time. I think I think all critical care providers are obsessive compulsive disorder people, they want results now.
They run towards the resuscitation, the code blue signal, etc., etc. So for people who like that, and they’re all here [gestures around him], this is an exciting place to be and sepsis is just a part of that.
Why is Sepsis a Problem
Khateeb: You gave us a great view from the top of the hill, but let’s kind of go deep into the valley in terms of what happens when we don’t find new ways to not only innovate but perhaps let go of old paradigms and dogmas and medicine.
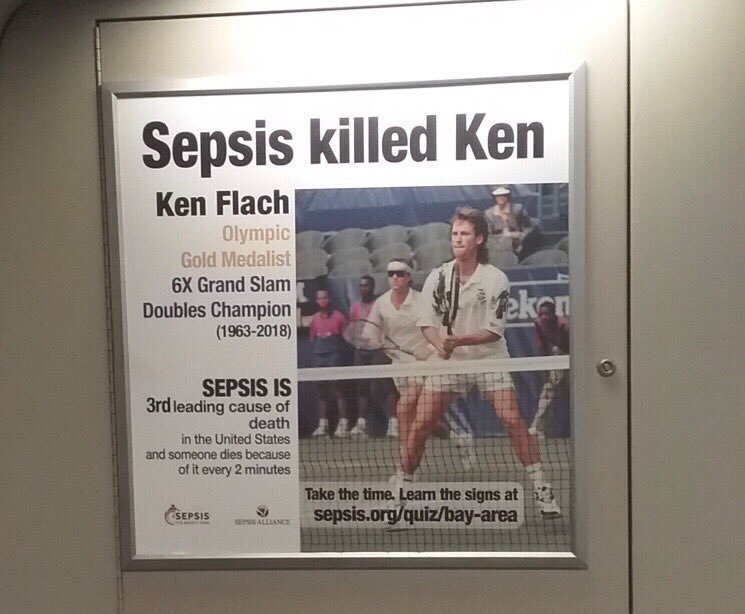
How bad does sepsis become? Because from my understanding, it’s at the level of a worldwide or global crisis for how many people it kills.
Zimmerman: Well, in fairness, the World Health Organization has made a difference in the last ten years.
But let me just preface that by saying that in 2019, every 3 seconds, someone in the world dies of sepsis.
Khateeb: Wow.
Zimmerman: And there’s a big burden, especially in children who are less than five years of age, are basically defenseless.
There’s a big burden on moms giving birth to children, a very high-risk group around the world.
And this has not only a huge impact on mortality, but we now know from adults and children who survive sepsis, is this does not go away.
There’s a big impact on how they live their lives. For children, we know at least a year old.
Khateeb: How does it not go away? Is it because it affects other organs in the body?
Zimmerman: Almost certainly related to the degree of organ failure when you’re really critically ill, your quality of life is affected.
You can’t think clearly, you don’t pay attention in school, you don’t go back to your job, you’re weak.
One of our ICU Heroes Award [recipients], Darrell Raikes, who was presented during the opening ceremony, came down with adult acute respiratory distress syndrome after knee replacement surgery.
This is years ago and he is still challenged physically, recovering from that incident that also involved sepsis. So now he’s a hero because he’s an educator and he’s an advocate for people facing post-intensive care syndrome.
Sepsis is sort of the gold standard for thinking about this. This problem does not go away when you leave the ICU or the hospital.
Khateeb: That’s a very interesting point because, I think, it seems that many decades ago, with medicine the idea was how do we best identify different pathologies based on symptoms and what we’re seeing and it seems that now we’ve gotten much better about it, because of technology because of the practice of medicine.
So now it’s more about how do we catch it before it happens? And then what do we do to intervene?
Can Sepsis be Prevented?
Zimmerman: Well
Is there a way that we can identify somebody with an infection before they transition to what we call sepsis? Which is an infection involving an organ dysfunction, which means this person now needs intensive care if it’s even available.
So that is a key question and the new Sepsis-3 criteria. I think there’s lots of controversy around it.
But personally, I like this new effort because there was actually an effort to talk about the way that we identified the at-risk patients with data, rather than people just sitting around and developing a consensus.
Which, with experts, is a good way to go about it as a first starting point, but these people who are involved in Sepsis-3 actually looked at data longitudinally over time, the patients in the ED [emergency department]…“He might have a suspicion of being infected and then sometime later, he ends up in the ICU with some type of organ dysfunction”…
So what were the predictors a few hours ago of what was going on with this patient that would have predicted we need to keep an eye on this person? Because he’s gonna have a high likelihood of being sick and needing critical care.
So these are all clinical criteria that we can measure, that a nurse or some other mechanism can get into the electronic medical record.
And we’ve improved but the area under the receiver operator curve for actually doing this in a good way is around 0.7.
So the specificity, the sensitivity are both improved maybe over our old methodology, but it’s still clinical criteria and there’s still lots of false positives, there are still lots of false negatives.
So you can talk about communities of patients, but for a single patient, “this” patient, before you’re projecting what that person is going to do, is still tough.
So there is definitely room in the future for sepsis for Sepsis-4 or Sepsis-5, for addition of other data input, power analysis of signals that just don’t look at a single point in time of a temperature or respiratory rate but over time.
There is an opportunity to look at the genetic makeup of this person who has a fever and because this patient’s genes are like this, “Whoa, we better pay attention to this because this person has a high risk of becoming hypotensive,” or actually looking at gene expression or protein expression in real time.
And this technology is just around the corner.
It’s going to happen in the next couple of years, where we can ask the question, “How is this patient responding to what looks like could be an infection?” We’re not sure whether it’s a bacteria or a virus but he certainly, kind of clinically, looks like he has an infection. Can we apply these other modalities of keeping an eye on his vital signs over time or getting a blood sample and
And we can improve both the sensitivity and the specificity of making a diagnosis of sepsis. And there’s no question about it, this will be technology that we will use in the future and it’s close at hand.
What is the Continuum of Care?

Khateeb: Now you mentioned something interesting.
With the Continuum of Care that has access to things like better genomics, it’s becoming more affordable.
On one side, we have
Is the next level in medicine to go beyond just sensitivity and specificity and perhaps whatever it would be in between? We’re not ruling out or not ruling in
Zimmerman: I view this more like a funnel.
Up at the top of that funnel, It’s okay to be overly sensitive.
But as we go down this funnel and we apply other things in addition to very simple clinical criteria, we might add in organ dysfunction, we might add in a power analysis of heart rate or blood pressure, we might add in a biomarker…
We take the larger group of patients that we are worried about and we quickly cull down to the population that’s at highest risk for something bad happening, for example, with an infection.
And those are the patients that we really need to clue into. So it is definitely a spectrum and everybody responds to an injury or illness like an infection differently, but we are learning now that it’s the host, the person, not the infection that ultimately really gets you in trouble.
And if we can define that better, I think ultimately we will be able to take care of patients sooner and more accurately than we have in the past.
Khateeb: Absolutely. So it seems that being more focused on, say if you have a hundred patients, not all one hundred them are going to be treated the same.
Not every person should be treated the same, right? But it sounds like what you’re saying is to be a lot more focused to identify the high-risk patients so that way the majority of energy and resources are dedicated to those, versus spreading it over a larger population who may not need as much focus and resources and just essentially getting more defined.
Zimmerman: Yes. And first of all I have to say, to put this in the proper perspective, this is an ideal state and that’s what we should be trying to achieve, closing this gap between resource-limited settings and countries who have everything is really what the whole of us need to be thinking about as we do our work in this area and I guess we have lots of evidence that technology gets less expensive as we increasingly use it.
The best example of what you’re talking about right now, you’re talking about personalized medicine.
Everybody’s talking about personalized medicine and I say, “Well great, but give me an example where we’re going to go with that.” Well, there’s two things that I’m very close to.
Treating patients with refractory hypotension, cardiovascular failure, and sepsis, I guess is the most common scenario. And the question for at least five decades has been, “Does this drug class, corticosteroids, the one we use nowadays is hydrocortisone, does this drug class improve outcomes?”
And there have been 20 or 30 adult trials.
If you do a meta-analysis of all of these four trials, on the forest plot in that summary diamond, you have to get your magnifying glass out. It is left of the line but it is almost kissing it.
So this is not a “Kablammo!” intervention. It helps, but probably in specific patients.
One of the groups of specific patients that I think adult investigators might say in terms of precision is patients who are sickest, who require the largest amount of support for their low blood pressure was sepsis.
This is the group that many people
And instead of exposing all of these other patients to corticosteroids, which further downregulates their adaptive immunity and places them at increased risk for not clearing the infection, reactivation of viruses, or getting hospital-acquired infection, just don’t treat that group with corticosteroids and get rid of that risk and really focus in on these much sicker patients.
That’s a clinical cut for precision medicine.
Then there is the genomic work and
So he has both approaches but to cut to the chase, he has identified kids with different endotypes based on their messenger RNA expression and if you plot this on a heat map, you can visually see these two groups of kids are different.
It’s easy to see based on the messenger RNA expression.
There’s this group here on the left and the heat map is almost blue. What does that mean?
It means that these genes are all down-regulated. What are these genes, Hector?
Many of them, maybe most of them, are related to adaptive immunity. So in one group of children with a specific endotype, giving steroids for their septic shock actually increases their risk of dying.
Whereas this other group who are not as down-regulated have a different endotype, different gene expression signature, these children actually can benefit from corticosteroids.
So that’s what the cancer people have been doing for a while and it’s very exciting. And this is just one little tiny snippet.
But that is a good example of
Usual Care in Medicine

Khateeb: That’s fantastic. Now we’re getting out of the valley, going higher up into the hills into a sort of a brighter future. You mentioned something earlier when we first met and I’m very curious to learn about it, but you mentioned this idea and correct me if I’m mistaken; “usual care.” Tell me about that.
Zimmerman: So usual care is the interdisciplinary team, I would say, with oversight from the intensivist who is helping provide leadership for this team, but a lot of focus on the infantry bed care providers, the nurses there, respiratory therapist there…this idea of “How do we provide this usual care for our patients?” And why is it that important?
If you look at children…in the 1950s, if you’re a child and you had a diagnosis of septic shock, your chances of dying were probably about 80%. Now, if you have pediatric septic shock and you’re treated in a Pediatric Intensive Care Unit and you have organ dysfunction, your risk of dying in the hospital is about 10%. We have no magic bullets that have come along during that time.
The only thing that has changed is how we provide this “usual care” to our patients. 50 years ago, nobody washed their hands when they are in
Khateeb: And then someone wise came around.
Zimmerman: Well someone wise came around, a hundred and fifty, a hundred years ago, and said we should be washing our hands. But I started as a pediatric resident. We didn’t wash our hands anytime we were in the room.
Khateeb: Interesting!
What is ABCDEF Bundle?

Zimmerman: There were still people smoking in the hospital, in the Intensive Care Unit when I started so we have made, with quality improvement, lots of changes.
Like we used to just assume that when you’re sick, you’re going to get secondarily infected because your immune system is mostly down-regulated and that was just sort of inevitable.
We put these central lines in and thought, “We’ll be careful, but they’re going to get infected.”
That thinking is completely gone now and in most hospitals, if you have a hospital-acquired infection involving a central venous catheter, this is a reportable event by that ICU and it gets reviewed in some detail and it’s a red mark with your care.
That is sort of prologue to saying the Society of Critical Care Medicine has helped support this idea, this program called ICU Liberation, the A-B-C-D-E-F bundle.
- “A,” always treat pain first
- “B,” undertake both a daily spontaneous breathing trial and a spontaneous awakening trial
- “C,” be cognizant of the choice of sedatives that you’re using
- “D,” monitor for delirium, try to minimize it by choosing your drugs correctly
- “E,” early mobilization, get that patient out of bed. Don’t let him sit there, that’s the wrong thing to do
- “F,” get the family engaged and empowered in the care plan
So in the last two years, there have been these two, I would say, landmark articles.
The first was by Marianne Barnes-Daly and colleagues from Southern California, published in critical care medicine and then this year, just very recently, Brenda
Two different studies that looked at this ICU Liberation implementation. And what they did is very clever.
They looked at the proportion of the bundle elements that were actually applied to given patients over their course in the Intensive Care Unit on a day-to-day basis.
And what they found was this dose-response relationship, the greater the implementation of these six bundle elements, the better the outcome.
Decreased risk of death, decreased
The signal for this intervention, it’s fair to say, given the limitations of maybe there’s a study design, this signal is bigger than any fancy new biologic or other things that we have done.
So we really need to pay attention to this and I think SCCM, for example, is taking this concept on the road.
It needs to be disseminated because there’s really strong evidence that it’s valuable and it makes sense.
New Approaches in Critical Care Medicine

Khateeb: Interesting. I have a couple more questions, again we want to be mindful of your time.
So, you mentioned some very exciting things coming out from SCCM and coming from the hard work of your colleagues. We mentioned Samuel Semmelweis earlier and for those who are not familiar…
Zimmerman: Ignaz Semmelweis.
Khateeb: Ignaz, thank you! Ignaz Semmelweis.
Zimmerman: My wife is a former infection control practitioner and this is their hero, I’ll tell you.
Khateeb: Yeah, he’s definitely a hero.
And for those who don’t know just a quick tidbit about him, his history, is that he introduced hand-washing a hundred and fifty years ago when it was not standard of care and showed that people were dying because physicians were not washing their hands.
But it wasn’t adopted until 20 years later. And there’s this cognitive bias called the Semmelweis Effect, where you reject new evidence because you are holding onto an old paradigm.
So with physicians and nurses who might be holding onto an old paradigm, how do you work together with the Society and your colleagues to help illuminate these new ways and modalities of treating patients? So that way it doesn’t take 20 years.
Zimmerman: Yes, the important fact is you recognize or identify a new intervention or approach,
Most people make their decisions on a variety of inputs but a big, strong one is their training and their experience.
Obviously, we don’t have evidence for a lot of things we do and that should be the gold standard and there are nice approaches that everybody respects on getting to the evidence basis, but I think what the Society of Critical Care Medicine does is, first of all, it has a forum once a year, a congress and I would say this is the largest congress of critical care. And I didn’t say medicine, I said critical care because it is interdisciplinary, the largest congress ever for critical care anywhere.
So people are brought together.
They have the audience ask a question.
There is this classroom situation where it’s turned around, where instead of the teacher addressing the students, the students provide the primary input acting as teachers.
Khateeb: Very active group on Twitter, we love it!
Zimmerman: Very active group on Twitter, another way of engaging people in whatever’s going on and the social media thing is now embedded in all of our journals too, Critical Care Medicine, Pediatric Critical Care Medicine, and the new journal, ICU Explorations.
The idea from the editors is to engage people in a discussion of how can this article, in a faster way, change practice at the bedside. Because this is what it looks like, this is what we should be doing.
Not the way we were doing it before.
The SCCM is an expert on developing collaboratives, so people trying to solve problems can come into a forum where they talk to each other and discover “Oh, don’t do it that way, have you thought about this?” or “We did it this way and we found this was challenging but if we addressed this, we could make it work.”
The SCCM is expert at that.
So there are all of these different approaches that really address the idea of, “Let’s be open-minded about this. Let’s be evidence-based as much as we can. And let’s have the discussion about where we should go next.”
About New SCCM President Dr. Heatherlee Bailey

Khateeb: Fantastic. One final question and we’ll let you go. I believe the new president is Dr. Heatherlee Bailey and I heard that you did a nice job of introducing in and helping to induct her. But any words of advice from a former president to the new president.
Zimmerman: Well Heather is going to be great. She’s a firecracker. She has lots of energy, she listens, and she’s always engaged and reaching out.
What’s unique about Heather, and it exemplifies again the interdisciplinary nature of the Society Critical Care Medicine, is that she is our first person from emergency medicine to be president. The reason that this is a big deal is that it fits in perfectly with the theme of this
So we talked about what happens to these patients after they leave the ICU and we really have a responsibility to these people after they survived their critical illness and even leave the hospital. We’re looking at ways that we can help get those patients back to their normal lifestyle.
But on the other end of this Continuum is public education, pre-hospital care…What are the ambulance drivers doing?
What are our colleagues in the emergency medicine doing?
And how we should collaborate with them to make this transition from the ED into the ward or into the ICU seamless?
Heather’s going to be an expert on getting that part of our job integrated into what we’re most familiar with and we need to be working on both things.
Khateeb: Absolutely. Well, thank you so much for taking some time with us. How can everyone find you on Twitter? I believe you have a Twitter handle, correct?
Zimmerman: I do have a Twitter handle, it’s @jerjohzimm. Melissa from SCCM pushed me into the Twitter world and it was a new experience!
Khateeb: It’s great, isn’t it?
Zimmerman: Yes, I went and kicking and screaming but came out saying “yeah, that was pretty interesting.” I think I had just about 6100 followers when I left.
And that was way up from where I got it from Ruth, the last president, and I’m sure it will exponentially expand but now I am on my own account, so I think I’m at 320.
Khateeb: Oh, we’ll help you get that higher, but that’s perfectly fine! Well, we really appreciate you spending some time with us and sharing some wonderful pearls of wisdom and a great look at the future. It’s very exciting
{kind=link}