Hills and Valleys Podcast Ep 3: Dr. Azra Bihorac, MD, MS, on How Acute Kidney Injury Should Be Treated
Hills and Valleys is a podcast that uncovers stories from leaders in healthcare, tech, and everything in between. Straight from the heart of Silicon Valley, we give you a look at the good, the bad, and the future, one episode at a time. Brought to you by Potrero Medical.
About Dr. Azra Bihorac, MD, MS, UF Health, University of Florida Division of Nephrology, Hypertension & Renal Transplantation

Dr. Bihorac is an internist, nephrologist, general and neuro-intensivist with a career-long clinical and research interest in postoperative complications, more specifically sepsis and acute kidney injury.
She also has an abiding interest in complex biological systems, human-machine interaction and the use of rapid analytic techniques to optimize unstable patient care in real time.
She completed a Masters in Clinical Investigation with an emphasis on advanced quantitative research and developed expertise in computational and statistical methods in outcomes research, focused on perioperative critical care.
Her K23 career award focused on the study of the biological and microcirculatory markers of sepsis and their use in developing early predictive models for organ recovery.
The results of her work formed the basis for one of the projects of the P50 award, which was granted to the University of Florida Sepsis and Critical Illness Research Center and on which she serves both as project leader and as Data and Biostatistics Core investigator.
She also led several large clinical trials and published extensively about the epidemiology and outcomes of perioperative acute kidney injury.
In the last two years, she has worked with experts in predictive modeling, medical informatics, and autonomic networks to establish a collaborative research partnership.
Their long-term goal is to build upon the unique proximity between the faculties in engineering, computer science, and medicine to implement advances in data science and engineering in perioperative and critical care medicine.
You can view her work on www.prisma-p.org and follow her on Twitter @ AzraBihorac
Listen to the podcast on any of the platforms below, watch the full video interview, or continue reading this blog to see the transcript.
- Interviewer: Omar M. Khateeb, Director of Growth atPotrero Medical
- Interviewee: Dr. Azra Bihorac, Chair of Clinical and Translation Medicine at the University of Florida
Khateeb: My name is Omar M. Khateeb, I’m the Director of Growth at Potrero Medical and I’m very delighted and honored to be sitting with Dr. Azra Bihorac. We’re coming to you from San Diego, California, at the Society of Critical Care Medicine.
Dr. Bihorac is a professor of nephrology in medicine at the University of Florida. And I’m going to defer to her to kind of expand a little bit about that on her bio and her background.
Why Nephrologists Attend the Society of Critical Care Medicine Conference.
Bihorac: Right, so why is it a nephrologist is at a Society of Critical Care Medicine conference?
I practice as an intensivist, I was trained as a nephrologist, and then at the time when I finished my fellowship, I moved from Turkey, where the main modality for treating patients with end-stage renal disease was peritoneal dialysis.
When I moved here in ’99, nobody was on peritoneal dialysis. Everybody was on hemodialysis.
So I had to switch my research interest and that’s when I became interested in acute kidney injury.
Dr. Azra Bihorac’s Education and Training

Bihorac: And after finishing my nephrology fellowship, I felt that as a nephrologist, I can’t really understand acute kidney injury because I’m not there when people developed it.
So I said I got to be there if I want to change the disease and I said I have to be an intensivist because that’s where AKI occurs the most, and that’s when I decided to do another fellowship in critical care medicine.
And when I finished that I stayed as a faculty member in the department of anesthesiology because they managed the surgical ICU at the
But my clinical practice remains in ICU, Intensive Care Unit; I do a little bit of consulting as a nephrologist but mainly I work as an intensivist. Obviously, I always wear both hats, right? But that’s my little background about why I’m in the ICU and why am I here at SCCN and – about why I care about kidneys in the ICU.
Khateeb: So my father happens to be a surgeon as well and he was a foreign medical student and came into his residency here in the US.
I think a lot of people don’t understand the difficulty and what it really takes to do that. Can you expand or share a little more about that?
Bihorac: Sure. Well, I finished medical school in the 1990s at
I lived in the northern part of Bosnia and escaped, thankfully, from my town and then, as a war refugee, went to Turkey. I was an intern at that time, I had graduated from med school.
So when I went to Turkey, I actually was able to start
She was the chairman of medicine and professor of Nephrology, and it was a very strong department for both medicine and nephrology and I fell in love with nephrology obviously. As I finished my medicine there, training, it was four years in Turkey as opposed to three years here in America. And then I started a Nephrology fellowship and I got a fellowship from the International Society of Nephrology to come here and study and do research.
Bihorac: So I moved to Gainesville, started my research, and then got political asylum because I couldn’t go back to Turkey and I couldn’t go back to Bosnia. So in order to practice medicine, I had to repeat all my training.
I first finished my nephrology fellowship, and then I went back and did internal medicine again, and then I did Critical Care Medicine. So when I got my first job, I was 40 years old and I finally got my first salary. Up to that
I always remember that if it wasn’t for my family working and helping me I would never be who I am, right?
Khateeb: Absolutely, and you must be very passionate about what you do because you went through it twice just to get to where you are today.
So you mentioned that you developed an interest in acute kidney injury. Now, in medical school and
Balkan Nephropathy

Bihorac: It’s interesting because the first you
And that part that is known for the disease called Balkan Nephropathy.
It’s an endemic kidney disease there because, later it turns out, because of fungus in the ground and the water. And people will just develop shrinking kidneys. So there was a disproportionate amount of people with end-stage renal disease. A lot of dialysis patients where I was working.
And you know as a medical student we were doing fieldwork to understand Balkan Nephropathy. So it’s really true, a lot of people think it’s like “Oh you really lived there?” Yeah, I did. And then, you know, before the war started in my town a lot of doctors left.
But I had just started my job so I have to stay because
She was very famous. There was a lot of research into peritoneal dialysis
KDIGO and the AKI-RIFLE Criteria
Bihorac: When I came here, acute kidney injury became so apparently important because every console we would have was an acute kidney injury.
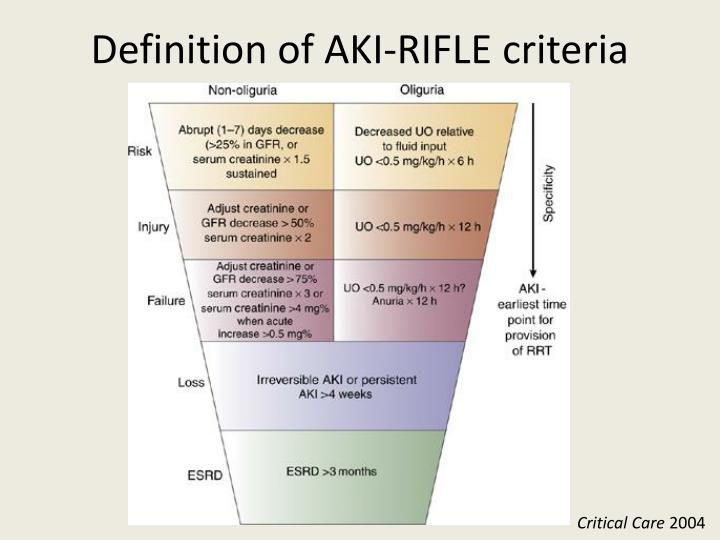
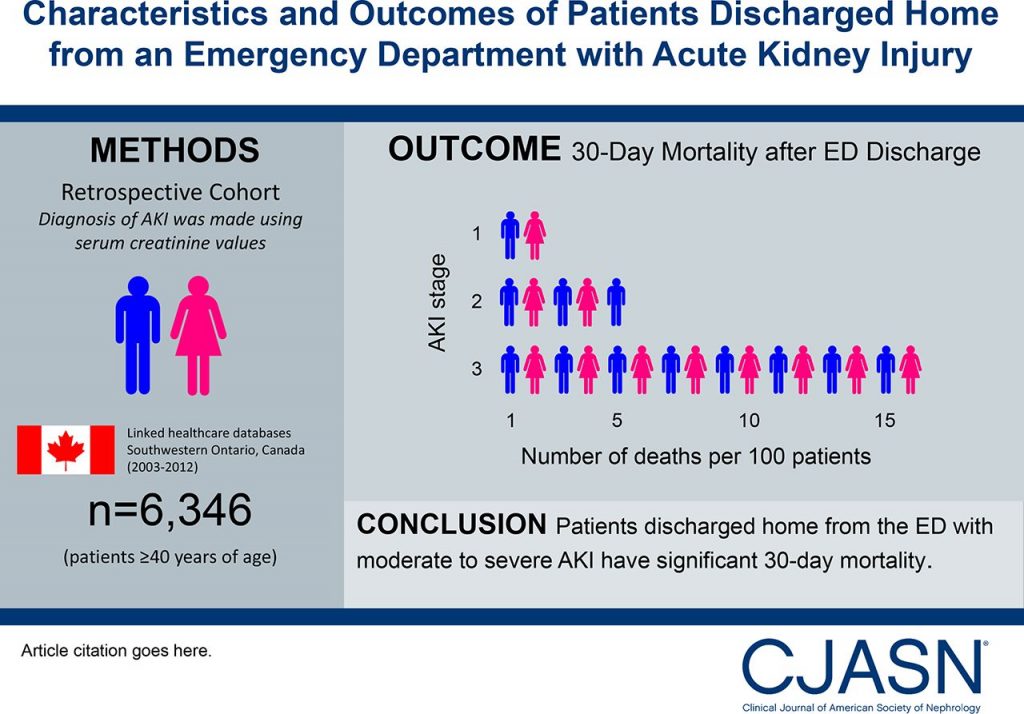
In 2004, I still remember that the RIFLE, the first consensus guidelines, came out on AKI. Up to that point only people who ended up having dialysis, the most severe stage of AKI, complete failure, would be considered as having acute renal failure. So if you consider only them it’s only 2%.
But when they publish the RIFLE criteria, Dr. Kellum and Dr. Ronco, it was around 2000. I still remember that paper, I was fascinated because suddenly you understood that there’s a whole spectrum, right? From mild to moderate to severe and I mean I was taken by that paper and wanted to understand in our own data how much, or how big is the problem? That’s kind of another interesting story.
So, you know, it was obvious when I looked at the data and we understood that short-term outcomes are prevalent and short outcomes are bad. And we wrote one of the papers on that and it was one of my first publications. But then, I became interested in long-term outcomes.
Like, in other words, you’re thinking it’s not just that you end up developing this acute kidney dysfunction that affects your outcome in the hospital, but perhaps even after you leave. You may still affect your outcome. We hypothesized this and at that time, nobody believed in that. Nobody. This was a long time ago in 2007.
And I finished Nephrology, I was doing internal medicine when my current boss, and he was one of my mentors, he was like, “let’s look at the long-term outcomes.” But at that time there was no electronic health record. There was no digital presence: like the labs, you know, we couldn’t get them in a digital way.
So what we did, we could get administrative data you could get, as an example, names of the patients and their ICD-9 codes.
Now if you know a little bit about claim data then you know that administrative code for acute kidney injury
How to Stage and Classify AKI
Khateeb: It goes under the radar I’m guessing?
Bihorac: Yes. So it’s not reported in claims. So the sensitivity of ICD-9 codes is at 20-30 %, 70 percent of the cases are never claimed and so if you want to use the RIFLE, you need creatinine.
So what we did is we got 10,000 patients that we knew who they are. We were interested in surgical patients, so we said let’s take patients who had surgery and let’s see what happened to them.
So first we’re going to call them and nobody would answer, that’s about 10,000 patients. We needed their creatinine and you couldn’t get them digitally.
So this is one of these weird stories that exist in life.
Bihorac: I was a fellow and in a critical care unit and then I had just become junior faculty and I wanted to do this project but, who’s going to get these creatinines?
And then there was a resident in anesthesia who ended up being on probation for some problems he had and they didn’t know what to do for him, and he was Turkish. That’s funny because they knew I came from Turkey and they were like, “you take care of him” because I used to live in Turkey like funny, right?
So they say, you mentor him and he’s your project now so, you know, do something with him. So
So he went into 10,000 records to write down creatinines in an Excel sheet.
Well, that’s a lot of work, we don’t need to do this anymore, but we did it then.
So we pull all the data and it showed that, and this paper was published in the annals of surgery, right, showing that AKI affects patient survival up to 10 years after surgery.
Even among the patients who never had kidney disease. So in other words, a look at the patients who had major surgery, they never had kidney problems before they come to the hospital, and after surgery develop a change in creatinine. Acute dysfunction or acute decline in your filtration function because it’s remote in organ dysfunction after surgery.
Bihorac: It happens in a lot of patients for
These patients, whether or not they recovered back to their baseline, did not do well up to 10 years after surgery day.
Their survival was lower in comparison to patients who never had a kidney problem.
This was the first time ever that somebody looked at that. And that was a paradigm change for a lot of studies later.
Acute Kidney Injury and Heart Failure
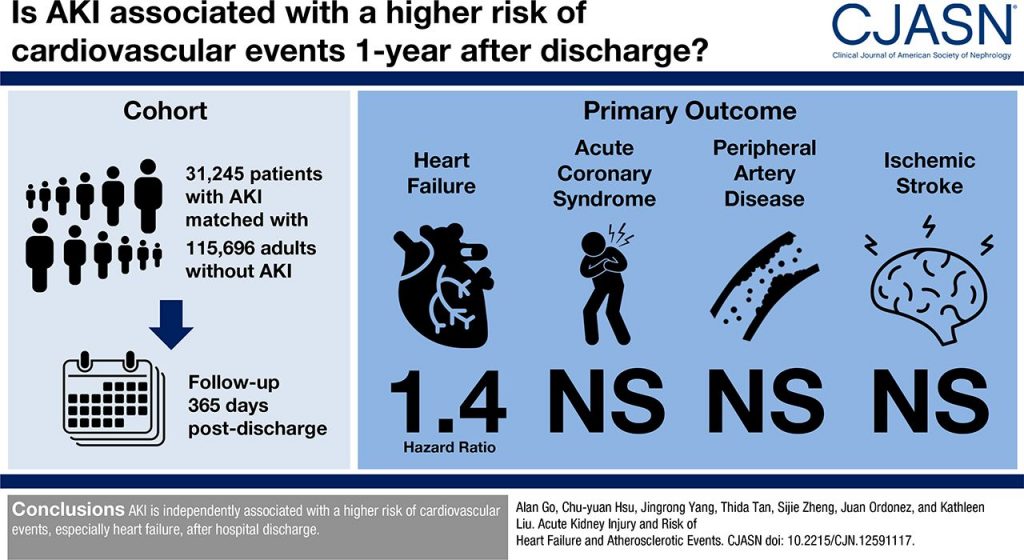
Bihorac: Now, we understand that it’s cardiovascular mortality that shows us that after AKI, 10 years after, you are two to four times more likely to die from cardiac disease and 4 to 6 times more likely to develop end-stage renal disease if you have acute dysfunction of the kidney, even if you didn’t have any kidney disease before.
Part of that is also the progression to chronic kidney disease, part of that I believe is a decline in your reserve and perhaps in endothelial health.
It’s all connected, but that was you know, that’s kind of one of those things.
Turkish people say it’s called Karder, you know? It’s your destiny, a good one, right? Here, things come your way because they are meant to happen to you and the little ducks came together.
Bihorac: So that’s how I became interested in
How is it associated with other complications? We need to change definitions reported in the surgical societies that report only more severe cases.
So we show that the American culture surgeon has a definition that misses a lot of cases of AKI that are not as severe but are still associated with bad outcomes.
That having acute kidney injury after surgery will still increase your risk for other complications like sepsis, mechanical ventilation, or being in the intensive care unit for a longer period of time.
So it really brought AKI on the radar, at least in my institution. But, if you move beyond where I work, it’s a one person mission. It’s very much a problem that there are not many people like me who do both worlds, right?
So what you have is a disconnect: if you think about all cases of acute kidney injury either after surgery or on the ward or in ICU in hospital, probably the distribution of the stages like mild would be 30 to 40% and then 20 percent moderate. And then very severe will be maybe ten percent of cases and maybe only 5% of which require dialysis.
So Nephrology will see those 5 to 10% of AKI cases. They are never called before.
People just don’t call them, for two reasons:
- Either they don’t really recognize it or
- they don’t think it’s important.
So, you know, it’s one of those interesting things and I always ask, why wouldn’t you consider calling?
They say things like,
“I thought it was just transient right?”
Or,
“Well, you know that people might be dehydrated”
and I say,
“Well I get dehydrated too but my creatinine doesn’t double!”
Right, I always get dehydrated.
The problem is that people tend to assign less value to that indicator.
I think they still don’t understand the physiology completely behind that.
A lot of that comes also from the biases in nephrology’s viewpoint of AKI, that the nephrologists themselves are those who are minimizing that.
So the problem’s reversibility, like is it reversible or is it not? If it’s reversible does it mean it’s completely benign?
We still don’t understand that because now we are seeing by the work done by Dr. Ronco that in patients who appear to recover from
Renal Functional Reserve and Renal Recovery
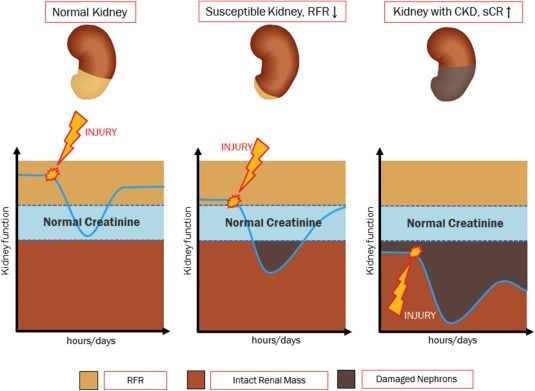
Bihorac: In other words: if you are born with two kidneys, you have the capacity to increase your filtration or clearance of the kidney up to almost 50 to 60 percent above what you operate usually.
So if you operate on a hundred percent, you can maximize to 160 percent when under the stress – when you need a lot of protein in the water or in
So what we now understand is as you age that reserve shrinks.
Khateeb: How much does it shrink by?
Bihorac: Well it depends, you know, not everybody’s the same. So basically, the vitality of the kidney declines with age, but not everybody declines at the same rate.
Just like not everybody ages the same way. So I think every organ in the body as a whole is in a slow decline, but the slope is different in different people.
So then certain diseases are obviously pretty susceptible to a much steeper decline like hypertension and diabetes. We know that. They are the most common in American society.
So now when you think about it aging has a slow decline, but in some instances, if you combine comorbidities with aging, then you get a perfect storm right now.
You have all these older people who might have some hypertension or diabetes. They don’t even know that and now they are going through all of these procedures in the hospital.
And now under the stress of acute illness, that inability to be resilient comes out in every organ.
And the kidney is incredibly susceptible to that.
Acute Kidney Injury Mortality
Khateeb: Unfortunately it seems that with nephrology, you’re only getting to see it when it comes to that 5% arrival score. When it’s already too late.
Bihorac: Exactly. And the thing is, those who see it before probably don’t know as much they should, they don’t necessarily know what to do.
And the nephrologists today, after all of these years of not being there, they don’t know what to do either.
So there is this gap now. There is this window where we need specialists for that population.
Some kind of crossroad in between an acute care doctor that can be a surgeon, internist, intensivist, and specialist for the kidney, which is the nephrologist.
So, that area of research is really something that I think needs to be emphasized more and more. Take me.
Khateeb: So, you gave us a wonderful view from
Take us a little deeper into the valley and I guess into the darker part where: if these things are not addressed and nephrologists are not getting a better look earlier on what AKI is, how does that put patients more at risk? And what does medicine look like if you don’t address these things?
Acute Kidney Injury and Sepsis
Bihorac: So I’ll tell you right now let’s take
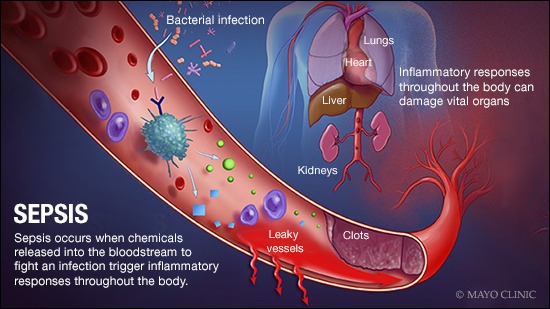
We all know it’s our top poster child, right? So sepsis, and we have
This dysregulated immune response to infection is associated with
You’re going to become hypotensive and your blood pressure is low, right? So we all focus very much in the cornerstone of sepsis, which is now to give fluids and antibiotics.
They have no therapy for it. All we do is we give fluid and we give antibiotics.
Khateeb: And they give fluid resuscitation, right?
Bihorac: Yeah, there’s a whole a lot of stuff right? So we give pressors, we try to maintain but we don’t necessarily have some thing that can cure sepsis. We have supportive therapy.
So organ dysfunction is now a main part of the sepsis picture. So I’m going to tell you like, say that we have a hundred patient with sepsis.
60 of them will develop acute kidney injury.
Okay amongst these 60 of one hundred patients, currently mortality in the hospital is in the range of 16% and 19%.
16 to 19 of those will die overall In the hospital.
They will not make it.
So let me guide you through who dies.
Among the hundred patients with sepsis, 60 will have acute kidney injury.
For those patients with acute kidney injury, 1/3 of them will reverse quickly; in the following forty-eight hours they will be able to reverse back.
The other 2/3 will have persistent acute kidney injury and will not be able to come back to their Baseline.
In the hospital, deaths occur for half of everybody who has persistent AKI and sepsis occurs in all of those patients. So if you die from sepsis, you will die with acute
kidney injury.
Khateeb: Can you repeat that one more time? So half of
Bihorac: Yes.
One in two patients with sepsis will have AKI to simplify.
One of those two with AKI will develop resistant AKI and will not come back to their baseline.
And half of those with persistent AKI will die in the hospital.
And of those who make it out, half of them will die within a year.
Khateeb: At what point during this process are nephrologists actually called in to check? How late is it?
Bihorac: Probably when you need dialysis and at that point, it’s too late.
So I think, and I always emphasize renal recovery.
First of all, in the first 48 hours, half of the patients have already developed AKI.
So in my opinion, those who can reverse quickly within 48 hours have a chance to make it.
So our first
Khateeb: That’s very true.
Bihorac: Just because it’s cheap doesn’t mean it doesn’t have worth, right?
But we all want to be heroes, you know, but sometimes we just need to be good workers.
So in the first 48 Hours, most of the acute kidney injury will be a combination of the inflammation associated with vasodilation, right?
And that’s when we give you fluid. In that first 48 hours of the sepsis, we give fluid and we give antibiotics, often we order tests.
We give antibiotics that can be nephrotoxic and we give tests that can be nephrotoxic, like contrast.
So if you pay attention to this and say, huh, I have patients with early AKI or higher risk for AKI, this is the patient that I need to treat differently than one who doesn’t.
This is the patient that I don’t want to give another
These are the patients that we focused on and that’s what we did in our research at
In other words: what we do right now is “All or Nothing,”
People who do everything or nothing are people who don’t really know what to do at the
Our tools to discriminate and find people in the mid-range of risk is very poor. So we can say well you’re doing great and you’re gonna, you know, recover great. Between dead and alive, we can distinguish those. In the gray area, not so much.
Khateeb: It seems that one of the big problems right now is that they just don’t have appropriate tools for this.
Bihorac: I’m really being an intensivist. Right now, nephrologists are not even at the
Khateeb: I think everybody’s very good at recognizing Aki but in terms of…
Bihorac: Not necessarily, not necessarily in the beginning.
We put a lot of value on hypotension and pulmonary function but in the early stages of AKI when we have maybe 20% to 40% to 50% increase, or 60% increase, we will just say well, this is just temporary or transient.
Not recognizing that this is the time when we need to make sure this does not persist.
Response Time for Acute Kidney Injury

Bihorac: So in the first 48 hours, try to reverse AKI if you can. If you cannot, and you have persistent AKI, it’s much harder.
Now we need to really look into the research that will help develop therapies for renal recovery.
And I’ll tell you now it’s not just intensivists.
This is now intensivists and nephrologists because, as of now, let’s add a problem.
Let’s say that you have developed resistant AKI. It’s more severe in new rounds, and you need renal replacement therapy. So some kind of support because your kidney doesn’t filtrate and you need dialysis.
Now think about it like a ventilator, right?
When you have a long dysfunction and you need oxygen to be supported by a machine, you get put on mechanical ventilation, but
However, and I think this is a big problem, one of the rare organ dysfunction
Chronic Kidney Disease and Dialysis

Khateeb: That’s true. And I’m seeing more of these at home dialysis machines.
Bihorac: In other words, the only chronic organ dysfunction that is currently sustainable is the kidney, because
People can live 10-15 years on dialysis after an organ transplant. So the only organ dysfunction that you can go from acute to chronic and be discharged home is with dialysis.
Now think about it: so you’re going to go from acute disease to chronic, and the doctors who take care of you for both acute and chronic are the same doctors.
All right, you see the problem? Not necessarily with bad intentions but like, most nephrologists are focused on chronic disease and how they manage a chronic dialysis patient.
That’s not the same right. I always say the number one goal for management of acute kidney disease that requires dialysis in
Clinical Decision Making and Cognitive Biases in Medicine
Khateeb: I want to bring something up that you mentioned. You’ve been very popular on Twitter, a lot of your slides have been very much tweeted about.
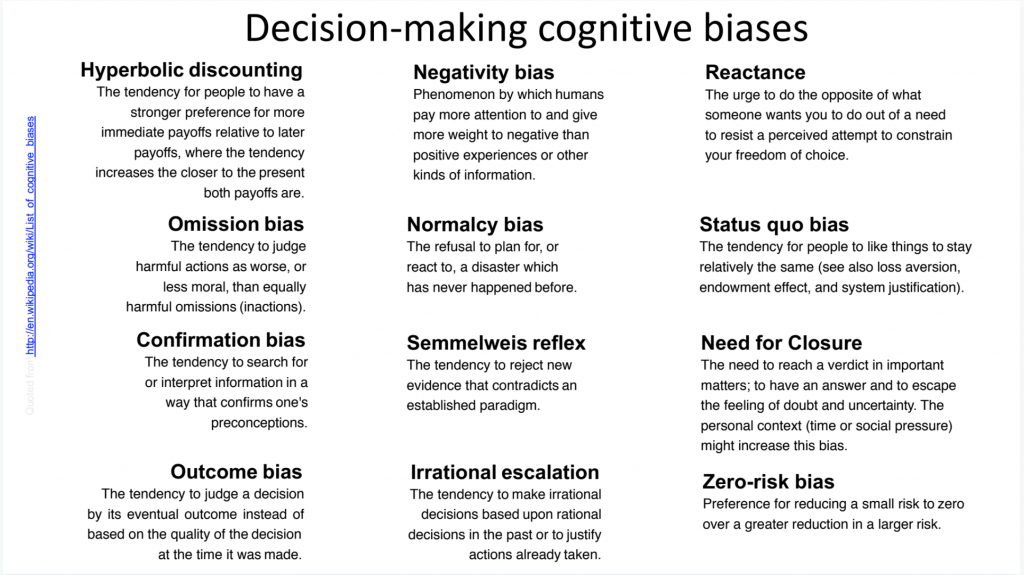
You had one about cognitive dissonance and cognitive biases and one was the Semmelweis Bias, which for our listeners who don’t know, Semmelweis was a physician who introduced washing hands early on in surgery and he was rejected by all of his peers and they thought that he was crazy.
This wasn’t accepted until 20 years later. The idea of this bias that she had mentioned was to reject new evidence that contradicts an established Paradigm. So, do you see that happening right now?
There’s new evidence that’s coming out, but a lot of the Physicians who are out there are holding onto the way that they used to be trained and the paradigms that they’re used to.
Bihorac: Yeah, the thing to think about is that the rifle was published in 2004.
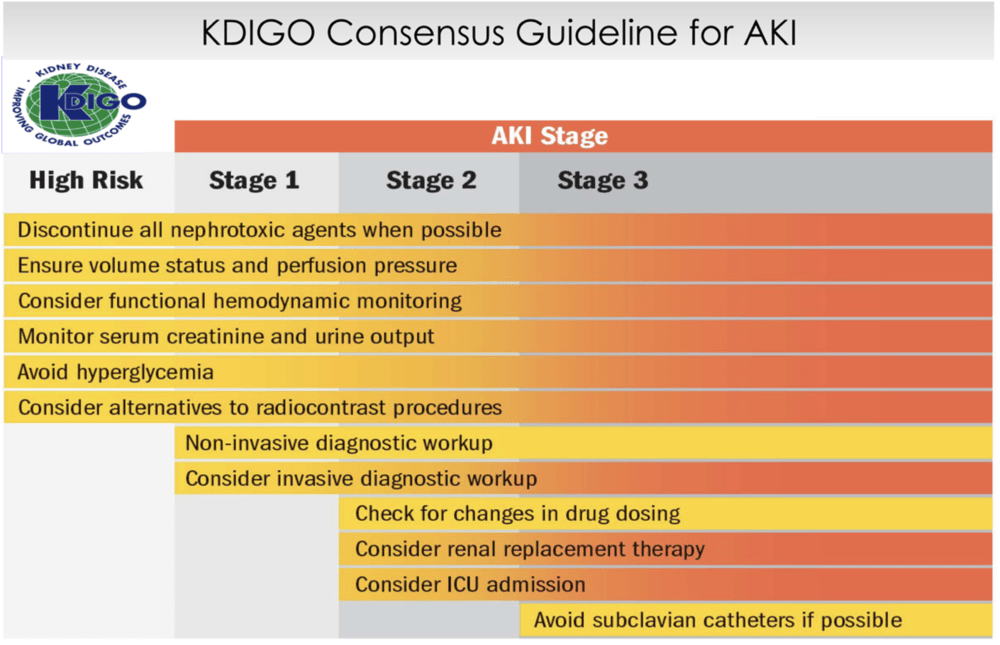
We are here 14 years later and people still don’t use it. Why is that? RIFLE and KDIGO consensus guidelines by nephrology societies are published and still exist.
Because again, it’s really hard to change beliefs. And all of this epidemiologic evidence that mild to moderate AKI, even if it’s transient, is associated with bad outcomes. That persistent is associated as well.
The problem here, there a couple, but the first one is that to use guidelines, one value of creatinine is not enough. The consensus guidelines define AKI based on a
So you really need to understand baseline function. So you need to use a little bit of your brain.
You need to put some work there. You need to go and think about well, what is your baseline renal function? What is, or what do I think your kidney’s health was before?
Okay, and you need to look at the records before. A lot of people don’t know about that, when you go to the doctor nobody tells you how your kidney health is.
No, they were gonna say your heart looks good, right? Whoever tells you how your kidneys look like? Never. Never.
It’s all about the heart unfortunately because we are so focused on certain organs. It is a culture of fixation on the heart and cancer and the brain.
What is, or what do I think your kidney’s health was before? Okay, and you need to look at the records before. A lot of people don’t know about that, when you go to the doctor nobody tells you how your kidney health is. No, they were gonna say your heart looks good, right?
Whoever tells you how your kidneys look like? Never. Never. It’s all about the heart unfortunately because we are so focused on certain organs. It is a culture of fixation on the heart and cancer and the brain.
Khateeb: But
Bihorac: Both patients and doctors don’t know.
The consensus guidelines exist, and you need to understand
Clinical Alert Notification Systems
Bihorac: If you look at the change of creatinine and then stage people accordingly, that’s hard. So right now we are working and we have developed something called “electronic phenotype” for acute kidney injury. Instead of
Dr. Kellum in Pittsburgh already has that alert; and in his institution, they saw, just by the fact that it’s reported there, a better outcome.
There are slight decreases in AKI. But Dr. Wilson in Yale did a study where they send a randomized alert to doctors on their pager saying, hey your patient has AKI.
One group would get alerts and one wouldn’t, and they looked to see what happened.
Guess what happened? Nothing.
Because doctors who got alerts and doctors who didn’t get alerts did the same thing.
There was no difference. They didn’t follow
When you ask them “do you follow KDIGO guidelines?” They say
Khateeb: Looks like the actions didn’t match the words.
Bihorac: Of course. Knowing is not acting.
It’s a very difficult problem.
It’s not just kidneys either, it’s many other things. Well, here’s another thing: so if you look at all cases of acute kidney injury in, let’s say, a
Of those hundred patients with AKI, about 7 out of 8 will not have any mention of AKI in their notes. It will never be mentioned in their notes, never.
So they’re gonna leave without ever knowing that they have AKI.
As a matter of fact, if you
Khateeb: And it’s because it hasn’t led to dialysis, is that the reason? So as long as you don’t need dialysis it’s fine – but they’re going to later on because it has gotten to such a bad point.
Bihorac: I mean, this is ridiculous, right? And it’s not going to be reported in the National Database because it’s not coded.
Khateeb: So if it’s not reported then there’s no problem. If there’s no problem, it continues.
Bihorac: Exactly. And then you’re going to leave.
I mean the data shows that 80% of patients who leave with AKI never get their creatinine measured. They leave the doctor and didn’t even know they had AKI.
Every episode of AKI puts you at higher risk for the next episode.
You can see these patients coming in and slowly developing chronic kidney disease, or dying, or having heart disease.
Because most of the time you will not end up on dialysis, you are just going to end up dying of heart disease.
So it’s a problem.
It’s an invisible disease that, for some reason, we have a problem assigning
And we don’t have a real owner. Right, and we don’t really have a report as any measure of performance. So it’s very interesting.
Khateeb: I mean it’s fascinating but it’s also very scary. We went very deep into the valley of how this can turn out.
I do want to talk a little bit about some of the great work that you and your team has been doing, but also if you can kind of take us “up the hill” and give us sort of a better look at this.
Like if this is addressed and we improve in terms of how patients are being treated and in the way that we’re looking at AKI, what could the future look? A brighter future than what it is, right?
How to Fix Healthcare

Bihorac: So first, in my opinion, we need to stop doing everything or nothing.
No more everybody gets everything or nobody gets anything right?
In other words, when you come with sepsis you don’t just get everything, and not everybody gets the same therapy. It makes no sense.
Because not everybody’s the same, right? Because you will over treat some people and
That means you’re going
Secondly, you harm people by doing too much, clearly, but then, on the other hand, we harm people when you don’t do enough.
So rather than doing too much or too little, we will just do the right amount of treatment for you. So that’s number one.
Bihorac: Number two. We need to utilize what we know right?
So how do you use the knowledge that you already have but just don’t know how to apply?
Because having knowledge and applying knowledge are two different things.
I know that I shouldn’t eat too much and I should exercise. But do I do that? No.
To the fault of myself, most of the humans hurt themselves, right? I mean, it’s well-known. The will power and the discipline, there is nothing like that.
So, you know, even as a doctor you want all of these things, but at the
We collect a lot of information on patients. It’s there with the digital electronic health records, information is there, but it’s absolutely ridiculously scattered and it’s overwhelming.
If you ever use electronic health records, there’s nothing appealing about them.
Digitalizing Medical Records

Bihorac: Digitalization is amazing, but as of now, doctors hate it.
Because as of now it’s not usable to doctors in a way that would help them or facilitate their decision making because it’s just a big spreadsheet in front of you.
You’re just inputting data like a paid data-entry person.
All of us: nurses, doctors, that’s what we do, right?
I mean it’s totally unfriendly, it’s based on very old programs.
We all know that. I still on my rounds have had people come in with paper and they are writing and I say, why do you have a paper?
Look, here is the data. Why do you need the paper? Just look at the screen, please. Stop reading from the paper.
We are such silly reductionists because we want to simplify things because that’s how we operate as humans.
We have to reduce
And then they will read read read read read you can you see read each patient file and describe parameters and I’ll say, okay, just answer one simple question: Is this patient better, worse, or the same as yesterday? Well, they cannot answer that question.
Khateeb: Why do you think that is?
Bihorac: Because it’s a really hard question.
That aggregation, you know, putting things in patterns in real-time, in a kind kind of temporal way is a very hard thing.
Especially in the intensive care unit.
So, as I say when somebody’s really doing well we can say they are improving. I think for the most part, the people who you think are stable, if you think they are the same as yesterday that means they are worse and you just don’t understand it yet.
Because in the ICU you can only get better; if you’re not getting better, you’re getting worse.
You’re just not catching it the moment when the patient goes down the rabbit hole. So that is really important.
And using that information from electronic health records to augment your decision-making in the ICU is the number one priority right now.
Causes of Kidney Failure

Bihorac: We have so many studies that we now know what constitutes a clinical risk for AKI. I mean the KDIGO published a study that says its susceptibility and exposure.
It’s a combination of your previous kidney health and exposure, acute exposure.
In other words, how healthy you are. If you are an older guy who has diabetes and hypertension, your kidney health is not going to be very good.
If you go in now and get sepsis, there’s a high potential you are not going to do well – you are high risk.
But you could be a young guy, but then you develop horrible septic shock and you get three bad nephrotoxic drugs that you get hammered by, then you can also develop AKI even though your health was good. So it’s a really big exposure or is it a combination of susceptibility and less severe exposure.
But still not everybody develops AKI, but now we have a biomarker; we have something that can biologically tell us.
So we combine the two. In other words, if you use a biomarker that is not
If I say, well not everybody needs a $50 or $100 test, maybe one day if it’s a dollar we will have it but as of now if it costs $100 for a test and I have a hundred patients. If I can test only 50 and got a lot more information than hand testing a hundred, why would I test one hundred right? So that’s what we do.
We say well we’re going to use clinical health records, or electronic health records to quantify your clinical risk.
Bihorac: If you are low
You are doing great. Please leave him alone, right? I mean, I don’t need to convince myself that you doing good. But if you have a high clinical risk, some of you will develop AKI and so now I will use a biomarker. If the biomarker is negative then I will still do nothing because it tells me that you had a clinical risk,
Khateeb: And those are the ones that are most complicated that need the most attention?
Bihorac: I need to focus on the kidney,
I’m going to say hey, you are gonna get creatinine every twelve hours, I’m going to measure urine every hour, you need a foley.
Not the other 75 patients, but you need a foley, you need your output hourly, you need an ultrasound to look at the fluid in you, and you need more monitoring.
You will not get Vancomycin, you’re going to get a more expensive antibiotic that doesn’t hurt the kidney because if I give you a nephrotoxic drug, you’re going to end up with dialysis, which costs thousands of dollars and you’re going to be dead.
So let’s save some money on what matters.
You need to defocus on the short-term to look in the future long-term.
Because you are not helping the person to leave the hospital, you are helping
So that is the problem, Health Care is so fragmented, right?
You have a doctor who sees 12 hours in surgery, then he gives you to a doctor who sees you for seven days in the ICU, and then as you exit you see another doctor before you leave the hospital.
But nobody is seeing you a year from now. As I say, we should all look at you and ask: how can I make sure that a year from now you’re living a fully functional life at the same quality you had before you came to this Hospital? That is the problem.
We need that for you. And for
Khateeb: This sounds like, and I know that you have a lot of experience with this in regards to your deep learning algorithm, that it’s trending towards predictive health to be able to predict how a patient is one year, two years, three years from now.
You mentioned focusing on the short term in order to have a long-term view.
So in the short
You said you will increase urine output and have more monitoring so that you have an influx of data.
Can you talk a little bit about the value of using technology to solve for that influx of data? Because I think physicians and nurses have this adverse reaction to more data because they have to manually manage it.
Bihorac: The problem with big data in medicine as of now is that it’s a big problem.
Challenges of Big Data in Healthcare

Bihorac: In healthcare, everybody wants the technology to be there but it’s not as simple as that. It’s not as simple as shopping on the internet.
The probability of harm and the price are higher, the complexity of the problem is immense, the dirtiness of the data is incredible, and the fragmentation of the data is even more ridiculous.
A lot of people think about this and I just live it every day.
I’m also board-certified in medical informatics and my whole research was in informatics and big data in healthcare.
But a lot of people still don’t understand. They say “oh, now they have all of this data so they can do all of these beautiful things.”
Well, first of all, let me stop you right there.
Think about data and where it comes from. How is data generated in medicine?
Where does EHR data come from?
It comes from different places, right?
So let’s say we just focus on the data that comes from monitors, in the ICU every patient is monitored by their vital signs, which is just blood pressure, your heart rate, your oxygen levels.
Just take those three.
So they are continuously monitoring patients on the monitors, and those monitors record data with a very high frequency: 60 hertz to 100 hertz, that can give you
That data is de-identified, it doesn’t have your name attached, it’s just numbers. The data comes from that monitor in a format that is protected by the company/hospital.
You can get it in
Let’s say it extracts from 60 hertz to one. So you just get one per minute.
Or let’s say that you had a hundred data points per minute being collected but you only get to see one per minute, which is still good. In the ICU now, when you are at the bedside you see the waveform.
And this is the most ridiculous thing I’ve ever heard. So now how does it get associated with you? How do I know now that that is your data?
Well, the way it works, at least in this system, is that the nurse at the bedside gets a spreadsheet and she associates you with the data point.
She picks up one data point and validates it, and the data is being recorded every 15 minutes, so you archive every 15 minutes by using manual validation from the bedside nurse. Is that ridiculous or what?
Khateeb: It’s taking an old problem and just putting a new hat on it.
Bihorac: How hard is it to have a tag on a
It’s
We still work in a room that has a million wires with bags that are a hundred pounds heavy.
You can’t move them, and when you want to go to a patient’s bed and get behind their bed, you need to move this big bag and move all of these wires. It’s ridiculous.
Who wants to be in this room, right? But the market is not open, the market is not a competitive market.
Khateeb: Do you see that changing now with companies like Apple and Google and Amazon and all these tech companies coming into medicine? Is that going to help? Is it going to complicate things?
Bihorac: I don’t know whether or not they will really come in.
It’s not so simple.
I think that the data as of now is not going to leave easily from your institution. The ownership of the data, the people who generate that data, doctor’s, hospital’s, patients, who does the data belong to?
Do they want to send it or store it in some cloud?
I’m not sure, but people understand that the data is very valuable.
I have a vision of what I call intelligent healthcare.
I think we have learned a lot about healthcare, we understand that there are biological determinants of care like the genome and protein metabolism.
We are now learning about precision medicine, with which we can predict models.
But I think that intelligent medicine is about the delivery of the care: how do you intelligently deliver care using technology to help you deliver?
Sequential Organ Failure Assessment (SOFA) Score and Machine Learning
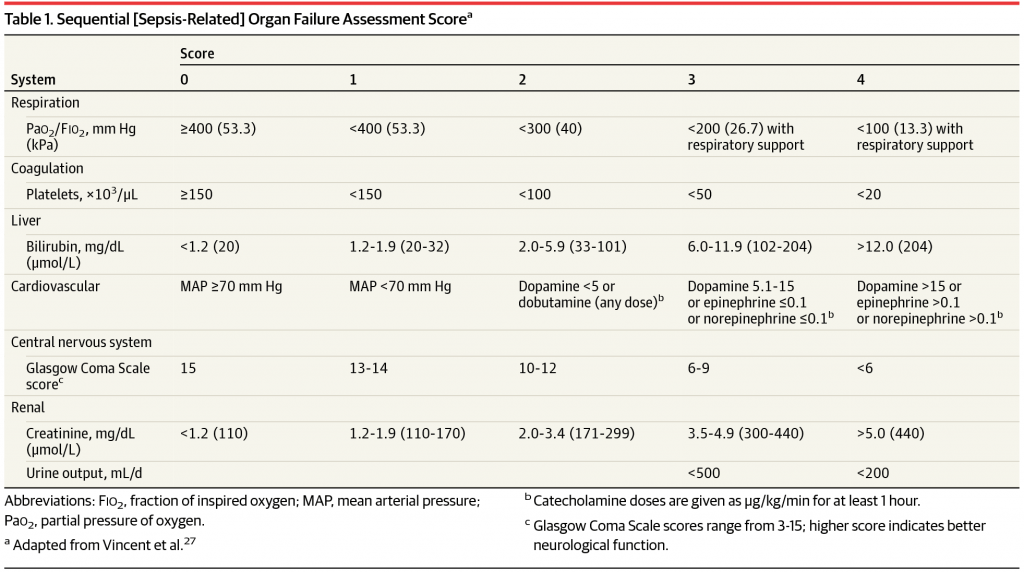
Khateeb: I want to touch on some of your work that came out because it was very exciting. Can you tell us a little about deep SOFAS and what does it stand for?
Bihorac: That’s one of our projects that we are trying to develop to use machine learning and to develop algorithms that can use all of these data points and predict probabilities of certain events.
SOFAS stands for sequential organ failure assessment score and is used in sepsis now to quantify organ dysfunction using 13 variables.
It’s
But you know, it simplifies things. It was meant to be
We have to pull Wikipedia out all the time even though it’s in their definition.
All of that knowledge exists, but it’s not used.
So we wanted to use the same information in an autonomous fashion so that the computer will calculate
In another way, it will point you to a time where you need to pay attention to events, because something is happening there.
That’s why the mortality risk went up.
So you go on, you do your triage, then use your skills to understand what’s going on.
Your examination, your visual, etc. Because as of now, your experience is irreplaceable by computer.
The computer is not there, you are. One day maybe computer will have that, but as of now only a human has that, and a computer doesn’t.
So that’s what we are trying to do, and we want to deliver that in the room. And we want to deliver that to your doctor, we want to deliver that to your nurse, we want to deliver that to your caregiver and to you as a patient.
We want you to see that, and we also want to see your trajectory. We want to see when you are green or yellow or red because the patient in current medicine is seen as a victim.
That’s how we see medicine: we see the human as a victim of the disease. But I want to see you as a protagonist.
This is your story.
No story ends well if you are the victim.
Only those who take action and become protagonists and directors of their own destiny do well.
Tapping into Healing Energy
Bihorac: We have never tapped into that potential of human healing that exists in us because we have healed without any doctors, we can heal ourselves and we absolutely don’t understand much about it.
I personally think the power of healing that exist in you as an organism, in your cells, we need to tap into that. I think the number one thing is to make the patient the protagonist in that story, and that movie is about him.
He becomes the center, he knows that he cannot leave in a black box.
That environment has to become enlightening, questioning everything that is done to you and working together with the doctors to get better.
Bihorac: I think that the root of this space that we are in has become dehumanized.
It’s not human-centered, It’s alienating. That needs to change.
Maybe one day your home will be your room, maybe you don’t even need to come to us, I don’t know.
I just kind of like to think about the future, about how we can change this whole Paradigm of healing and medicine one day.
Khateeb: Do you feel that Predictive Technologies, and let’s take deep SOFAS as an example: when better technologies come out, you help the physicians and nurses be their own protagonist.
And if they can be
Bihorac: Absolutely. Most of the time now Healthcare Providers are data entry people.
There are studies showing that 80% of their time is spent charting, even in the ICU.
80% of the time an ICU nurse is charting, 20% for direct patient care. So that means the 80% of the time you are not observed in a hospital, in the intensive care unit.
You are unobserved, you alone. And that’s another project we are working on currently: that not just intelligence or AI is needed, you need pervasive sensing.
You need an environment that senses you 24/7.
Hospital Room of the Future
The room is a part of the care delivery. We have a very simple system where we use a kinetics camera on the patient with an accelerometer, a sensor of the light and the noise.
And I can tell you that the low noise level in the ICU, the white noise level, is three times above WHO recommendation for the healthy noise level.
Also the light level. The light level has absolutely no pattern, no circadian rhythm.
It’s too dark in the day and it’s too light in the night. The patients are constantly interrupted in the night.
That’s why we have an issue with delirium in the ICU. That’s why people go crazy in the hospital.
I mean know
We also use VR in our interventional trial.
How easy it is to give patients VR? They love it just to relax when they are stressed. So these little things that we can use could make a huge impact.
It’s not all about this being a drug-centric, procedure-centric healing process.
It doesn’t tap in your regenerative capacity, it doesn’t tap into your mind or in your spirituality. None of these.
Khateeb: And these are all things that have shown over time to be a huge help.
Bihorac: Of course, and guess what? [00:58:00] We just like drugs and procedures, because it is a
Khateeb: You keep mentioning and it keeps popping up where it’s either acute or chronic, good or bad.
And it seems like the old way of medicine, and maybe the old way of
But where we really should be living and understanding things is in this gray area that you mentioned: the continuum.
Bihorac: Their health is not acute and chronic, it’s only one “health”, right? And you need to see it as a Continuum.
Khateeb: That makes a lot of sense. There’s an old quote that says: the person who looks at another being and says that they are either a God or a monster forgets that night and day are still one.
It seems that this is the same way with medicine patients that, as you were saying, it’s a Continuum.
Do you see the hospital of the future
Bihorac: Yes, and it never stops.
It exists in your home and exists after you leave. I think we will become smarter in understanding the changes, starting with before, then acutely, then when it’s more intense, and then again when they leave. There is no reason that we should stop watching.
How is our blood pressure performing? How is our heart rate in a recovery period? This is very important
Patients even in the hospital go from being in the ICU being watched by one nurse for one patient. He gets a little better and they send him to the floor where one nurse watches eight patients, and some people don’t get seen for four hours.
Well at that point, it’s better to be at home. We don’t have any good transitions and we don’t have this big world view from above.
I think that it will require the restructuring of our understanding. The fragmentation of medical care on every level: on a data level, on a monitoring level, on a health delivery level, and on the workforce level – the fragmentation is the problem.
Empowering Patients in Their Own Care

Khateeb: Absolutely. This concept that you mentioned about making the patient a protagonist instead of a victim, to see themselves as a protagonist of the story I think is a very powerful narrative.
Do you see that with a lot of these consumer tech companies that are coming up with wearables and stuff that if they do the right way, they can educate the population to be that protagonist and take more charge of their health?
We’ve seen since the arrival of the internet and WebMD that patients are more educated when they go see their doctor. How do we continue to close that roof so it becomes more of a Continuum?
Bihorac: That’s a great question. I think it’s really important. I think we need to open the black box of hospital care, and continue to educate patients. I mean medicine is a privilege. Being a doctor is a privilege.
And it’s a challenging profession. No question about that.
And I think that you we try to control quality by punishing errors, not by fixing them.
It’s punitive, and I’m not sure that’s the best way to do it. I think empowering from inside, both doctors and
And it’s an interesting concept. I’m by no means a health care reform specialist or anything, but I live in it. I see how hard it is for both doctors and patients.
And I always tell my patients to be loud.
Stand for yourself and speak for yourself, because patients have power but they often don’t use it.
They are also in this kind of conservative environment where whatever doctor says, that’s what it is.
And that can be nice; it’s nice to trust, but I think that kind of paternalistic approach is something that we need to step away from.
Khateeb: They have to be the protagonist and stand on their own two feet. Maybe they need to look at the doctors and nurses in the hospital as tools rather than the heroes and heroines. It’s a very interesting concept.
Bihorac: Partners, they are all Partners. That’s how I see it.
I mean we see that even in the gender distribution in medicine, that kind of old way of paternalistic medicine.
It’s very hard to abandon, but slowly the influx of women and younger people who don’t carry that image of male culture will result in it changing.
Khateeb: They say that the hand that erases is the only hand that can write the truth. So what does
Bihorac: That’s a great question. I think it first needs to admit vulnerability, right? I mean it has to admit that sometimes there is nothing to be done.
And it’s okay to say that. I think it also has to admit that it is not mechanistic delivery of drugs or procedure, it is healing.
It is about healing and it’s about human connection.
We are all going to die as of now, maybe we live 200 years or 300 years but I don’t think we will be immortal.
So I think that medicine needs to embrace death first in this society. And also embrace that instead of preparing for that. We are just trying to run away from that.
And we hurt each other even more.
So we don’t optimize dying at all as of now, and I don’t think we can optimize healing if we don’t optimize dying – they all connected?
It’s a continuum, it’s a life, right?
I also think that rather than being reactive, we must become proactive. We start thinking about our health when we are born, and we very much invested in a healthspan concept starting with the young people.
Because longevity will start when you are healthy not when you are
Bihorac: But in the current market and in the current concept, there’s no money to be made in preventive medicine.
Probably at some
It’s not about money at that point. I think that is another hard concept.
Khateeb: Do you think it’s possible where maybe the new paradigm is helping people to optimize the continuum of life and health instead of treating the disease?
Bihorac: Perhaps, yes. The question becomes: is health a privilege or is it a right?
Having a healthy life, I believe it’s a right, but it’s also a responsibility. Because nobody’s going to give it to you. You’re gonna work for that yourself.
Khateeb: I guess the big theme about this is, as you mentioned before, about being the protagonist and taking responsibility for it.
Bihorac: Yes. And doctors need to educate patients about that even more and start very young.
That’s where technology can play a huge role. I think people now understand more and more that exercise and self-monitoring of the diet play a huge role, and it’s really starting to resonate with people.
It’s a different generation and it’s fantastic and this generation needs to step up and kind of look for new paradigms.
It’s not going to be your dad and your mom and it shouldn’t be, they need to argue and we need to ask more.
Khateeb: Well, I have to say it was an honor and a privilege. Very very insightful and I think you gave us all a lot to think about.
So doctor, thank you so much. Now real quick, I know that people are going to ask so I have to: how can people best find you?
Bihorac: Yeah, you can follow me on Twitter and I constantly wanted to write more, like I have this blog called Kidney Love.
It’s still not very active, but I’ll figure it out and I’ll let you know. Amazing to me is that not a lot of doctors are interested in health and wellness and all these new crazy ideas.
So there are some amazing ideas among people who are not doctors and there are good ideas that we need to put those two worlds together. And that’s what I like to do. And I also like to give a list of pros about life and love and
Khateeb: Fantastic. Well thank you for taking time with us Dr. Bihorac

{kind=link}